It is difficult if not impossible to square the current Congress’s recent attacks on health care with its responsibility to provide for the general welfare. Not the welfare of the wealthiest 1%, but the general welfare.
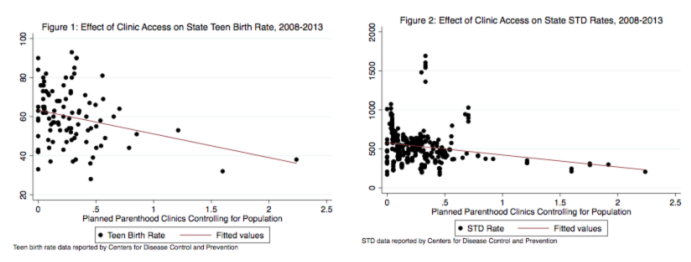
For a number of reasons, I have felt alienated by my current government. I am a woman, and like many other women across the country, have not taken kindly to the current Congress’s assaults on access to women’s health care – whether through Planned Parenthood or essential health benefits – sometimes without the input of any women. Women comprise 51% of the population, and any efforts to undermine our full inclusion in discussions about the care of our own bodies is as absurd as it is offensive. And my own research has shown the immense public health, and in turn economic impact that Planned Parenthood clinic access has for millions, driving down rates of STDs, teen pregnancy, and HIV. Gutting Planned Parenthood funding doesn’t make America great again, it makes teen pregnancy great again.
I am a rape survivor, and like many survivors of assault was appalled by the Republican Party’s normalizing of then-candidate Trump’s boasting of sexual assault, and am even more appalled by their treatment of sexual assault and domestic violence as declinable preexisting conditions under the American Health Care Act (AHCA).
The AHCA, which passed on May 4 with a mere 217 votes, is the most recent, and by all accounts most egregious grievance. And as with issues pertaining to women’s health, I have dual responses – those of a frequent patient, and those of a scholar whose work increasingly addresses health care policy.
As a scholar, I trust data, and while the House failed to wait for a CBO report, we know from the prior iteration that at least 24 million will lose coverage, and that many will face higher health costs on account of their being older, poorer, sicker, or (gasp!) born with a vagina. We know that the estimated premium hikes for those with asthma are $4,000, for those with diabetes are $5,500, for pregnancy are $17,000 (ironic given Republicans’ constraints on contraception and abortion), and for cancer are a whopping $140,000.
Cancer does not discriminate between Democrats and Republicans. It afflicts the young and the old, the rich and the poor, the liberal and the conservative, and we owe it to ourselves as a nation to care for individuals in need. And from an economic standpoint, we know that contributing to the nation’s economy is hardly as feasible when people are not physically or emotionally well. We know that while people will be grandfathered in to plans, 85% of people stop working when they receive cancer treatment, resulting in gaps in coverage that would lead them painfully vulnerable under this plan.
Moreover, by undermining essential health benefits and protections for those with preexisting conditions, this includes mental health treatment, which is essential for treating both mental illness and substance abuse amid a rampant opioid epidemic. And we know that mental illness and poverty are all-too-commonly linked, such that the economic impact of restricting access to care in this domain is devastating. Moreover, full-time employees with depression miss nearly twice as many work days each year than do their non-depressed counterparts, a pattern that could potentially have consequences resulting in gaps in coverage and in turn, the effect of changes to preexisting condition provisions.
While I have never had cancer, I have struggled with chronic illness from early childhood onward. With chronic kidney infections and ear infections, scarce were the days I wasn’t on an antibiotic. Throughout my teens and early twenties, I struggled with severe anemia with a then-unknown cause (it was later determined to be an autoimmune gastrointestinal condition), which ultimately required iron infusions. My final year of college, I was hospitalized for severe electrolyte abnormalities ultimately diagnosed years later when I was in graduate school (it is a rare parathyroid condition). With several subsequent hospitalizations, as well as ongoing depression and PTSD, I have for now several years had several doctors overseeing my care, with my survival (not to mention thriving) contingent upon taking a job that has good medical benefits in close proximity to high-quality research hospitals.
It is both dismaying and offensive that Representative Mo Brooks views those with preexisting conditions as being at fault for their conditions, for not leading good lives. With multiple autoimmune conditions, and extensive childhood illness, there is little question that I would have been in the 27% well before I could be blamed for what I eat or drink. And even if it were lung cancer, don’t patients deserve some measure of compassion? Are we so soulless that we are unwilling to help people to heal?
If we measure a country not by how it treats its wealthiest 1%, but rather by how it treats its most vulnerable, the Republican Party has a lot of explaining to do.
For a number of reasons, I have felt alienated by my current government. I am a woman, and like many other women across the country, have not taken kindly to the current Congress’s assaults on access to women’s health care – whether through Planned Parenthood or essential health benefits – sometimes without the input of any women. Women comprise 51% of the population, and any efforts to undermine our full inclusion in discussions about the care of our own bodies is as absurd as it is offensive. And my own research has shown the immense public health, and in turn economic impact that Planned Parenthood clinic access has for millions, driving down rates of STDs, teen pregnancy, and HIV. Gutting Planned Parenthood funding doesn’t make America great again, it makes teen pregnancy great again.
I am a rape survivor, and like many survivors of assault was appalled by the Republican Party’s normalizing of then-candidate Trump’s boasting of sexual assault, and am even more appalled by their treatment of sexual assault and domestic violence as declinable preexisting conditions under the American Health Care Act (AHCA).
The AHCA, which passed on May 4 with a mere 217 votes, is the most recent, and by all accounts most egregious grievance. And as with issues pertaining to women’s health, I have dual responses – those of a frequent patient, and those of a scholar whose work increasingly addresses health care policy.
As a scholar, I trust data, and while the House failed to wait for a CBO report, we know from the prior iteration that at least 24 million will lose coverage, and that many will face higher health costs on account of their being older, poorer, sicker, or (gasp!) born with a vagina. We know that the estimated premium hikes for those with asthma are $4,000, for those with diabetes are $5,500, for pregnancy are $17,000 (ironic given Republicans’ constraints on contraception and abortion), and for cancer are a whopping $140,000.
Cancer does not discriminate between Democrats and Republicans. It afflicts the young and the old, the rich and the poor, the liberal and the conservative, and we owe it to ourselves as a nation to care for individuals in need. And from an economic standpoint, we know that contributing to the nation’s economy is hardly as feasible when people are not physically or emotionally well. We know that while people will be grandfathered in to plans, 85% of people stop working when they receive cancer treatment, resulting in gaps in coverage that would lead them painfully vulnerable under this plan.
Moreover, by undermining essential health benefits and protections for those with preexisting conditions, this includes mental health treatment, which is essential for treating both mental illness and substance abuse amid a rampant opioid epidemic. And we know that mental illness and poverty are all-too-commonly linked, such that the economic impact of restricting access to care in this domain is devastating. Moreover, full-time employees with depression miss nearly twice as many work days each year than do their non-depressed counterparts, a pattern that could potentially have consequences resulting in gaps in coverage and in turn, the effect of changes to preexisting condition provisions.
While I have never had cancer, I have struggled with chronic illness from early childhood onward. With chronic kidney infections and ear infections, scarce were the days I wasn’t on an antibiotic. Throughout my teens and early twenties, I struggled with severe anemia with a then-unknown cause (it was later determined to be an autoimmune gastrointestinal condition), which ultimately required iron infusions. My final year of college, I was hospitalized for severe electrolyte abnormalities ultimately diagnosed years later when I was in graduate school (it is a rare parathyroid condition). With several subsequent hospitalizations, as well as ongoing depression and PTSD, I have for now several years had several doctors overseeing my care, with my survival (not to mention thriving) contingent upon taking a job that has good medical benefits in close proximity to high-quality research hospitals.
It is both dismaying and offensive that Representative Mo Brooks views those with preexisting conditions as being at fault for their conditions, for not leading good lives. With multiple autoimmune conditions, and extensive childhood illness, there is little question that I would have been in the 27% well before I could be blamed for what I eat or drink. And even if it were lung cancer, don’t patients deserve some measure of compassion? Are we so soulless that we are unwilling to help people to heal?
If we measure a country not by how it treats its wealthiest 1%, but rather by how it treats its most vulnerable, the Republican Party has a lot of explaining to do.
 RSS Feed
RSS Feed